


VO2 Max of Bodybuilders
Your VO2 max is the maximum rate of oxygen consumption your body can attain during intense physical exertion. The absolute VO2 max is expressed in L/min of oxygen consumption and can be measured by a bicycle or treadmill ergometer test while wearing a mask designed to measure oxygen consumption and CO2 production. Your VO2 max is a measure for your cardiorespiratory fitness, which turns out to be a strong, independent, and modifiable risk factor for a plethora of health threats such as premature death, cardiovascular disease, type 2 diabetes mellitus, and cancer. Other strong, independent, and modifiable health risk factors are smoking, visceral fat mass, and muscle strength. But the main health risk factor is age, which is unfortunately to date still unmodifiable.
Your VO2 max is determined by how efficiently your body can take up oxygen to produce energy, and thus depends on the efficiency of your lungs, heart, blood/vessels, and muscle mitochondria where oxygen is used to convert glucose and fat into energy for muscle contraction. Although partly genetically determined, your cardiorespiratory fitness (and thus VO2 max) can be significantly improved by physical activity, especially endurance training combined with high intensity interval training (HIIT). Low intensity endurance training will mainly improve mitochondrial efficiency to consume the oxygen in the muscles, whereas HIIT will mainly improve peak cardiac output (= heart rate x stroke volume) to bring the oxygen to the muscles. Stroke volume can be increased by training, whereas maximum heart rate (HR) is not modifiable and gradually decreases with age (about 1 bpm per year). Since stroke volume is inversely proportional to resting heart rate, HRmax/HRrest is a useful measure for peak cardiac output. Mitochondrial efficiency and peak cardiac output are both main contributors to VO2 max, but for most people peak cardiac output is the limiting factor. For untrained subjects, however, mitochondrial efficiency can also be a limitation factor.
VO2 max measurements are very popular among endurance athletes to get an idea about their condition and to compare it to previous measurements or results from other endurance athletes. As this has been the main use of VO2 max tests and because the absolute VO2 max obviously depends on body size, endurance athletes typically use relative VO2 max values, obtained by normalizing the absolute VO2 max by body weight, expressed in terms of the volume of oxygen consumed, per minute, per kilogram of body weight (mL/min.kg). Although this is an incorrect way of scaling for comparing VO2 max between humans of different sizes according to the theory of geometric similarity (refer to Scaling VO2max to body size differences to evaluate associations to CVD incidence and all-cause mortality risk, Eriksson JS, et al., BMJ Open Sport Exerc Med, 2021), it is an approximation that works rather well for endurance athletes that typically have a comparable body mass index (BMI=weight/height2 in kg/m2) and are mainly interested in their performance potential to move their body mass as fast as possible from point A to point B. After all, carrying less weight requires less energy and therefore makes you faster.
But what on earth can you do as a bodybuilder with a relative VO2 max / weight (in mL/min.kg), if you know that with every % that your body weight increases due to muscle hypertrophy, your relative VO2 max / weight decreases by the same %? The fact that relative VO2 max / weight (in mL/min.kg) is wrongly biased against higher body weights (heavier persons being penalized with lower values and lighter persons favoritized with higher values) makes it indeed useless to compare cardiorespiratory fitness between people with different BMI. Two persons of the same height and cardiorespiratory capacity, but different body weight will have the same absolute VO2 max (in L/min) but different relative VO2 max / weight (in mL/min.kg). Thus, using relative VO2 max / weight (in mL/min.kg) for people with a BMI that deviates significantly from the population's mean (e.g., bodybuilders, under- and overweight people) is inappropriate when comparing to reference values.
That body weight is not a good factor to normalize VO2 max for body size is quite obvious. Or have you ever seen a 120 kg person run as fast as a 60 kg person? Indeed, it are not the heavyweight bodybuilders and sumo wrestlers (with lots of muscle and/or fat mass) who have the highest absolute VO2 max values thanks to their high body weight, but rather the lightweight long-distance runners and cyclists (with little muscle and/or fat mass). But yes, a person who is 1.60 m tall could run as fast a person who is 2.10 m tall, otherwise all champion distance runners would be giants. So indeed, height is a meaningful parameter that can be used to normalize VO2 max. According to the theory of geometric similarity, persons of different body size/height (but with the same body shape and composition) will also have proportionately different sizes of lungs (total surface area of alveoli for O2 and CO2 exchange), heart (pumping capacity), blood volume (total amount of hemoglobin for oxygen transport), blood vessels, muscles (total size/volume of muscle mitochondria for oxygen consumption).
The correct way to normalize the absolute VO2 max for comparing the cardiorespiratory fitness of people of different size, in accordance with the theory of geometric similarity, is to scale it by the body height squared, giving relative VO2 max / height2 (in L/min.m2), which is a similar approach as used to compare the body weight of people of different height by using the BMI (in kg/m2). This is a much better measure for cardiorespiratory fitness, because absolute VO2 max obviously depends on body size (height), but not purely on body mass (weight) because changes in fat mass and muscle mass (due to fat and muscle cell atrophy or hypertrophy) do not change cardiorespiratory capacity proportionally (no meaningful impact on size or efficiency of lungs, heart, blood/vessels, or number, size, and function of muscle mitochondria). With atrophy or hypertrophy of fat cells, it is simply the amount of lipids in the fat cells that changes, and with extreme weight gain, possibly also the number of fat cells. Since fat cells do not provide energy for physical exertion/muscle contraction, this will have no impact on the VO2 max in any case. With atrophy or hypertrophy of muscle cells, it is mainly the amount of water and proteins (size of myofibrils) in the muscle cells that changes, and possibly also a small bit of glycogen storage. The number, size, and aerobic efficiency (function) of mitochondria in muscle cells are not necessarily affected significantly by muscle cell hypertrophy or atrophy.
Then the question remains why, according to the theory of geometric similarity, should you normalize with length2 and not with length or length3? This may be less intuitive but can also be understood by the fact that the surface area or cross-section of the biological structures or organs is particularly important for the speed of gas exchange and gas transport (total surface area of all alveoli, cross-sectional area of the heart and blood vessels, total binding surface area of all hemoglobin, total surface area of all muscle mitochondria). In addition, statistical evaluation of epidemiological data has confirmed that relative VO2 max / height2 (in L/min.m2) is properly associated with the health risks of interest.
As cardiorespiratory fitness (VO2 max) is very important for general physical condition and health, it is recommended to develop it as much as possible, preferably starting at early age. This can be achieved by regular endurance training combining (minimum 80% of) steady state Zone 2 training with (maximum 20% of) high intensity interval training (HIIT). For example, 4 to 5 times per week 45-90 minutes of steady state Zone 2 training at 65-80% of your HRmax plus 1 or 2 times per week HIIT with 4 to 6 intervals of 4 minutes at 85-95% of HRmax and 4 minutes recovery. A reasonable alternative could be to do 4 to 6 times per week 45-90 minutes of steady state Zone 2 training at 65-80% of HRmax where every other day (i.e., 3 or 4 times per week) the last 6 minutes of the session are done at high intensity (85-95% of HRmax). This type of training approach could increase your absolute VO2 max after 6 to 24 months with 10-20%. Although I have never seen any data about it, I hypothesize that sufficient training in higher HR zones (80-90% of HRmax) could possibly slow down a bit the gradual decline in HRmax observed with aging.
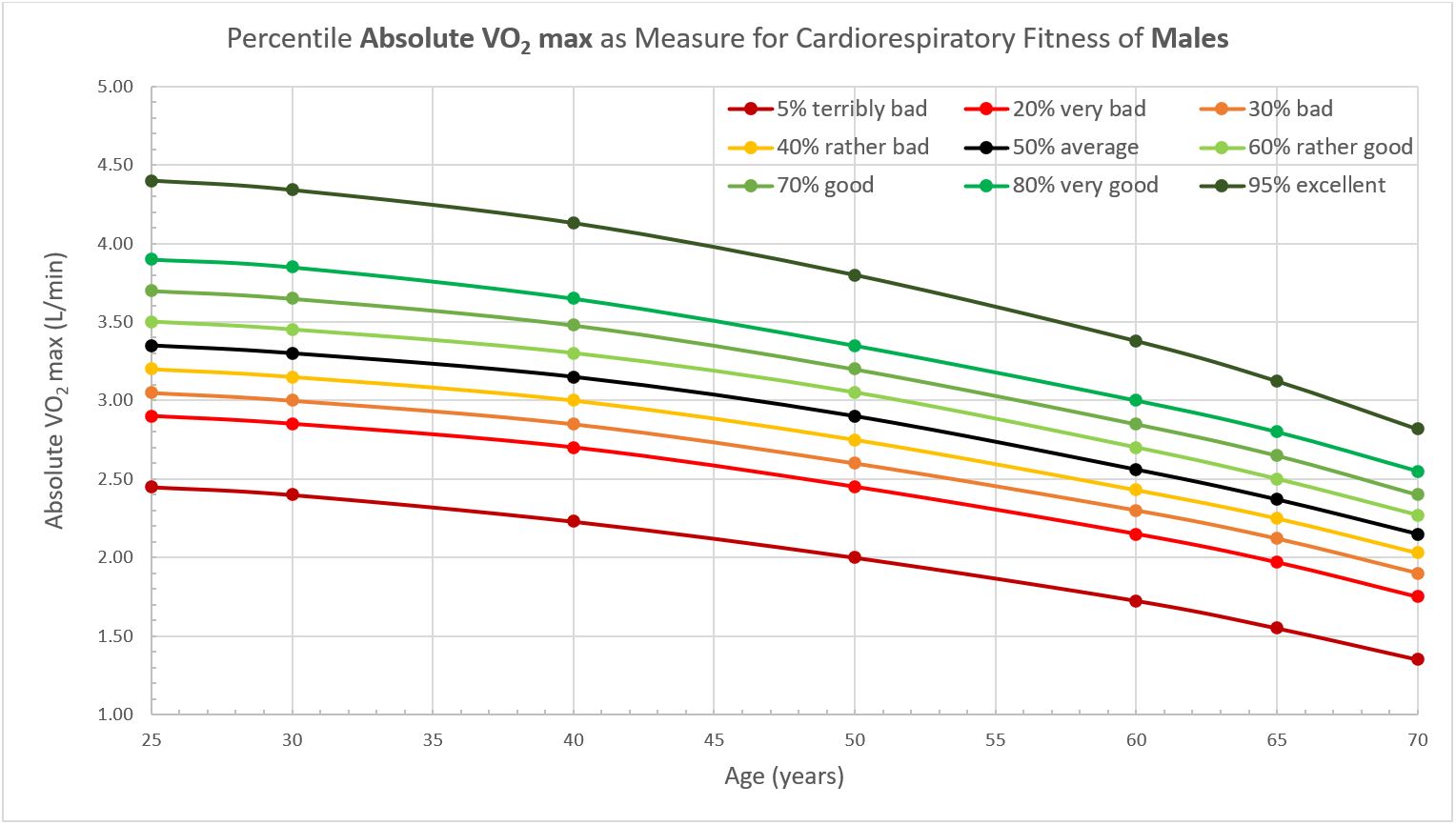
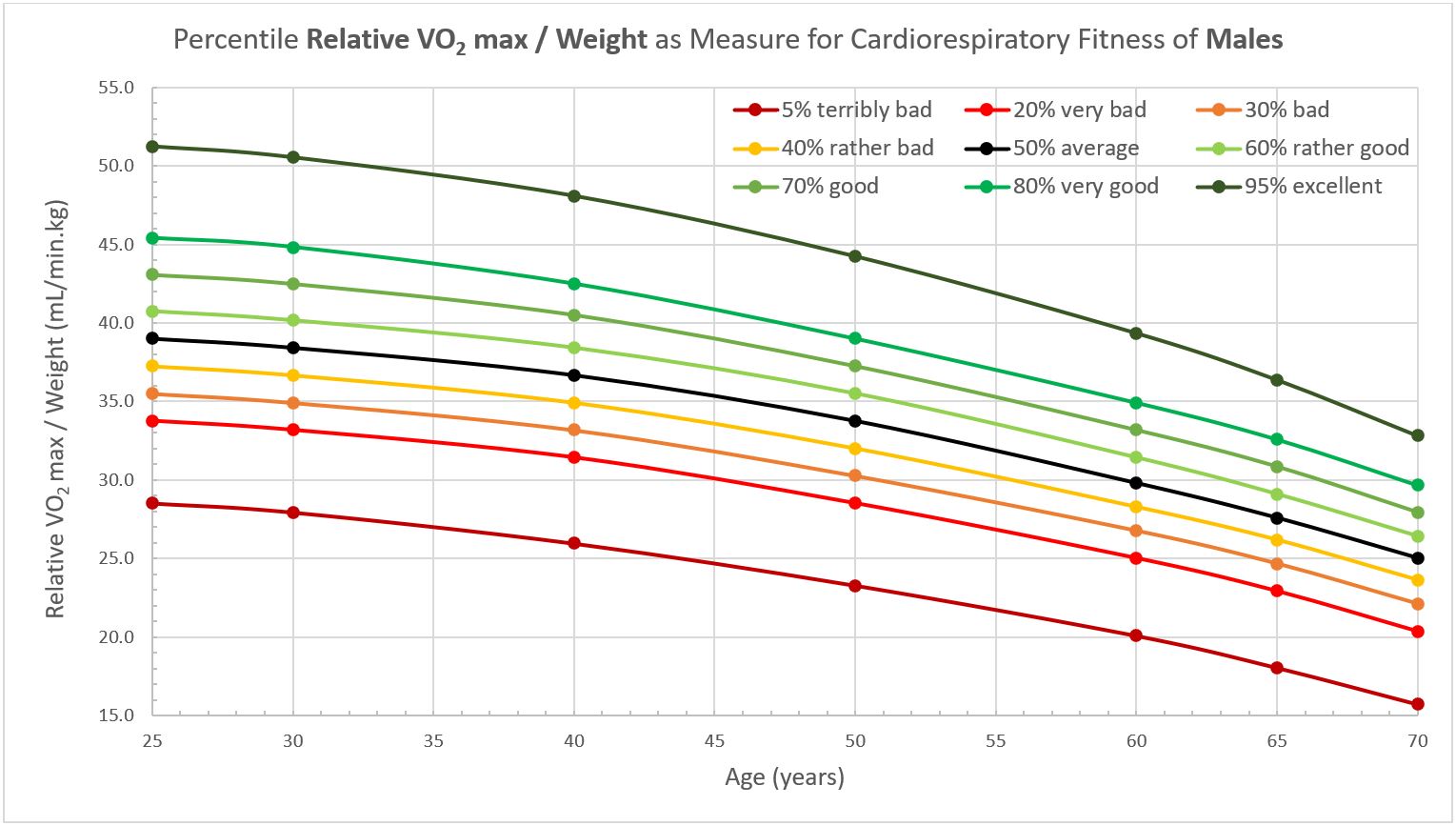
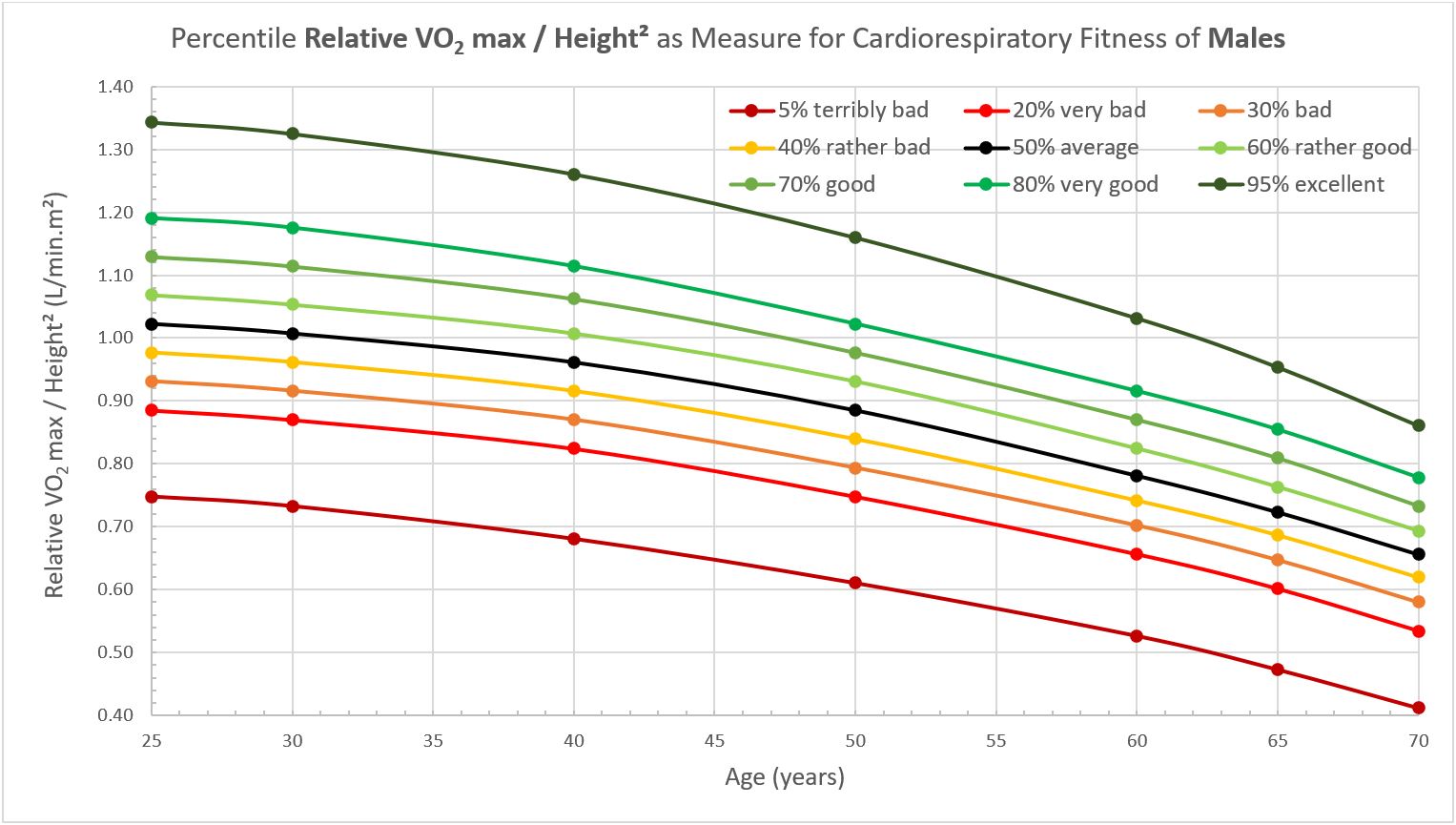
VO2 Max Reference Charts for Males
Below you find charts with reference values of VO2 max for males as measured by a cycle ergometer-based incremental cardiopulmonary exercise test (data based on Reference Values for Peak Oxygen Uptake, Rapp D, et al., Dtsch Z Sportmed, 2018) and expressed as absolute VO2 max (in L/min), relative VO2 max / weight (in mL/min.kg), and relative VO2 max / height2 (in L/min.m2). The participants were 6,462 healthy German men of average height 181 cm, average weight 85.9 kg, and average age 46 years (ranging from 21 to 83 years).
Notice that in all 3 graphs the VO2 max rapidly decreases as people age. This decrease in VO2 max with age also occurs in endurance athletes who continue to train throughout their lives, albeit at a slightly slower pace. So, age is a key parameter influencing your cardiorespiratory fitness. The absolute VO2 max (in L/min) is dependent on the person's height, the relative VO2 max / weight (in mL/min.kg) is dependent on the person's weight, and relative VO2 max / height2 (in L/min.m2) is independent from the person's body size (height and weight). So, people should compare their VO2 max with people of similar age, and especially if your body size (weight or height) differs significantly from the population's mean, one should use the relative VO2 max / height2 (in L/min.m2) for meaningful comparisons.
Note that the HRmax you can reach by running on a treadmill is typically 5 to 8% higher than by cycling on a stationary bike and in untrained subjects the VO2 max test results on a treadmill can be 5 to 20% higher than on a cycle ergometer because a larger muscle mass is involved in treadmill ergometry and because cycle ergometry is often terminated early due to locale muscle fatigue (refer to Updated Reference Standards for Cardiorespiratory Fitness Measured with Cardiopulmonary Exercise Testing (FRIEND), Leonard A, et al., Mayo Clinic Proceedings, 2021).
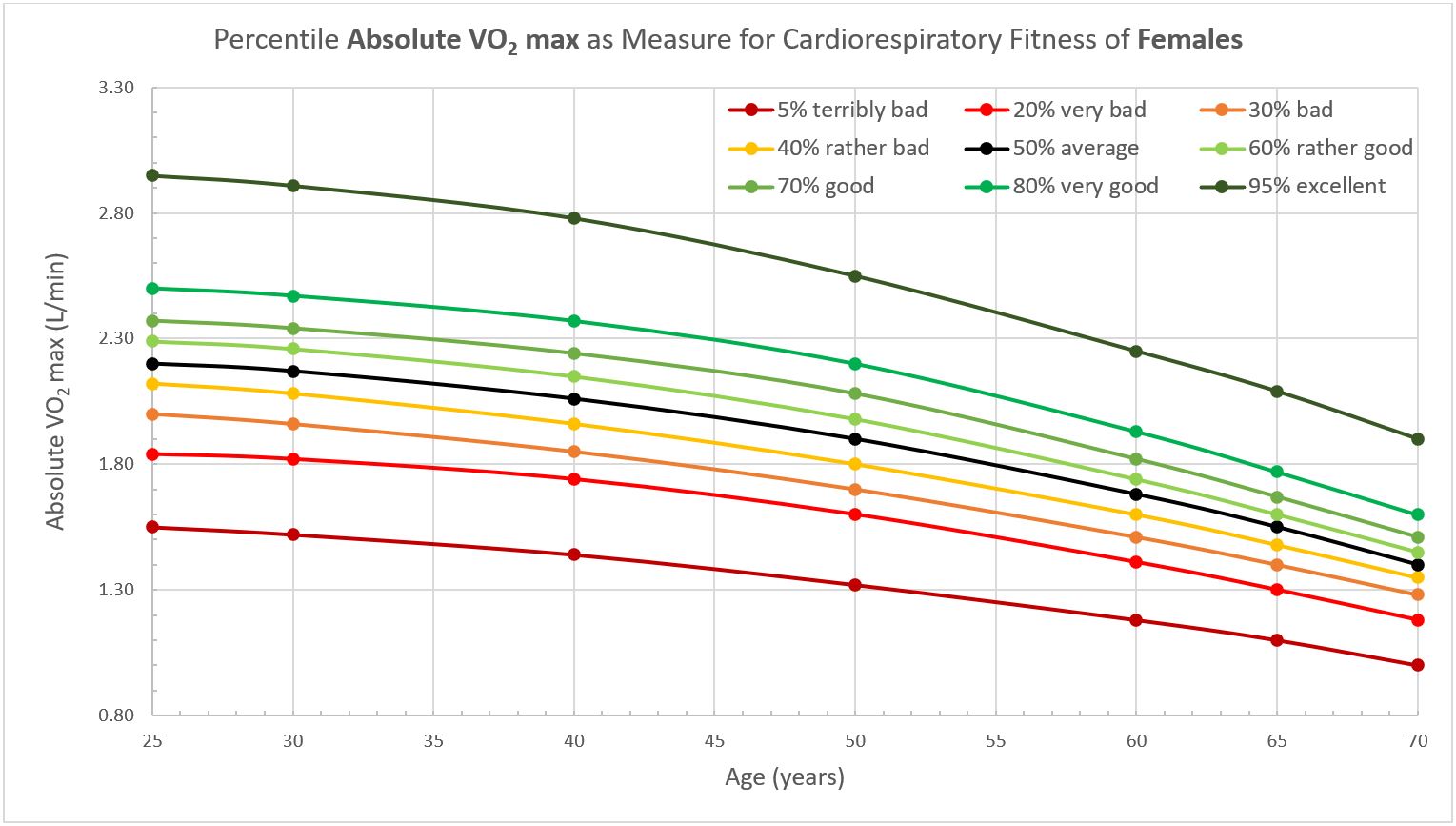
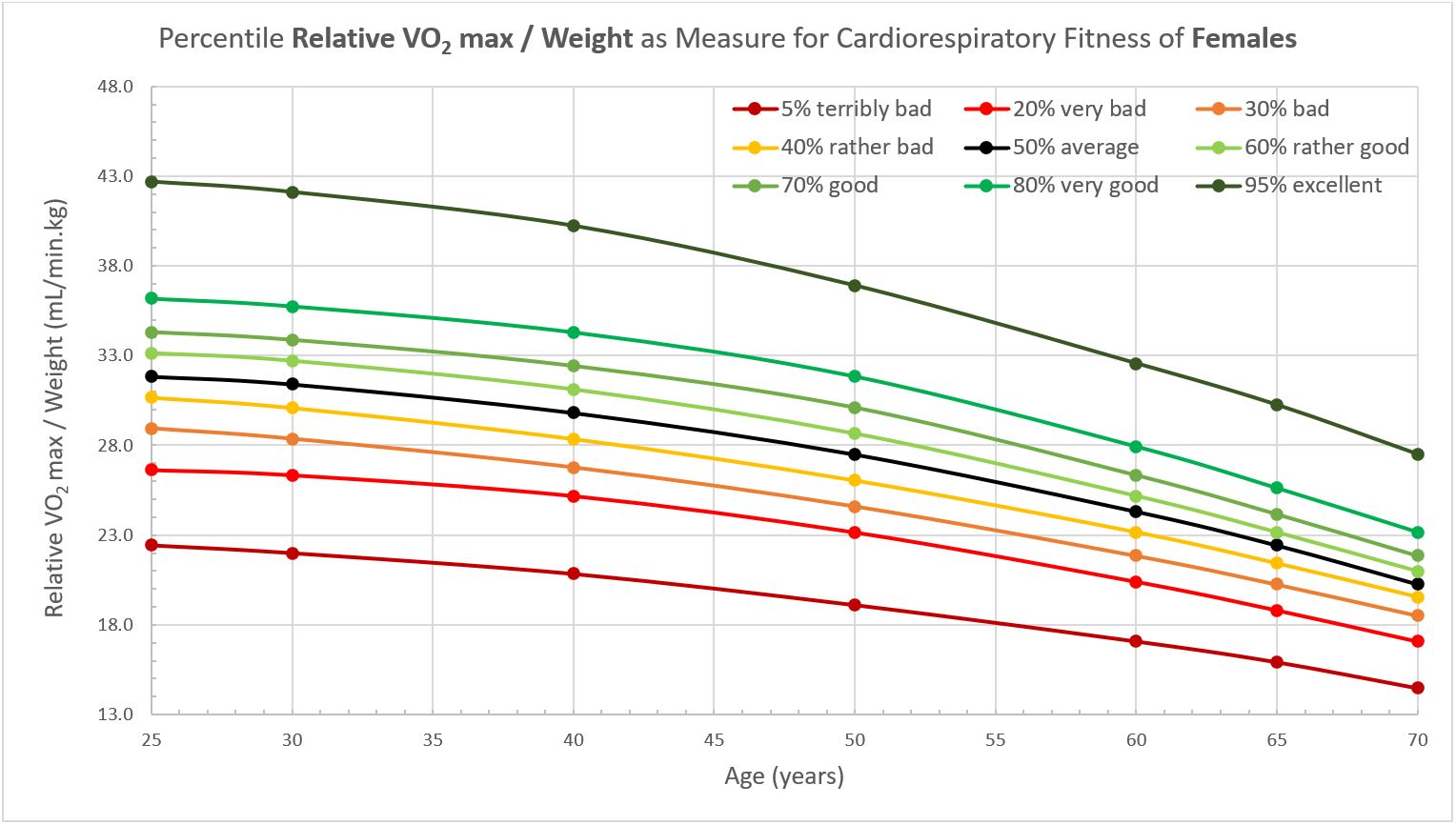
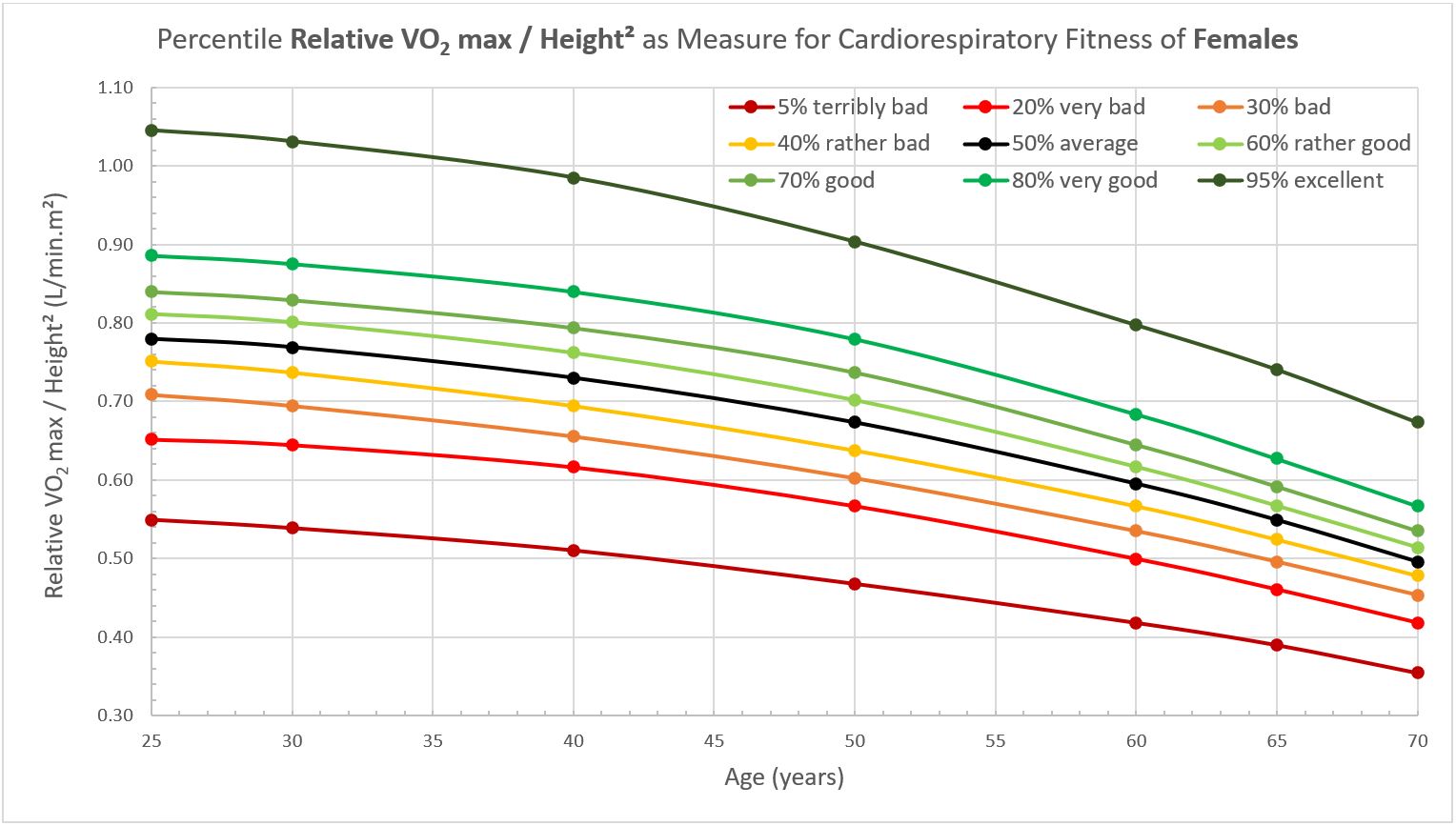
VO2 Max Reference Charts for Females
There is, however, one other very important parameter that has a major impact on your measured VO2 max result, and that is your gender. Females have a significantly lower VO2 max than males: women typically have an absolute VO2 max (in L/min) that is 35% lower, a relative VO2 max / weight (in mL/min.kg) that is 20% lower, and a relative VO2 max / height2 (in L/min.m2) that is 25% lower than men. Below you find charts with reference values of VO2 max for females as measured by a cycle ergometer test. The participants were 3,628 healthy German women of average height 168 cm, average weight 69.1 kg, and average age 46 years (ranging from 21 to 83 years).
Conclusion
When used correctly, VO2 max tests can be a very useful tool to measure your cardiorespiratory fitness, which is a very important contributor to your general health. Your VO2 max is, however, very much dependent on your sex and age, regardless of being expressed in absolute terms (L/min) or in relative terms (mL/min.kg or L/min.m2). Obviously, absolute VO2 max (in L/min) also depends on body size: a giant can be expected to be able to consume oxygen at a higher rate than a dwarf of the same sex and age. Therefore, if you want to compare your VO2 max to that of people of different size, your VO2 max needs to be properly normalized for body size. Since changes in muscle mass and fat mass do not per se impact your ability to consume oxygen, and thus your cardiorespiratory fitness, a normalization based on body height is more appropriate than a normalization based on body weight.
To illustrate this, the table below shows a comparison of the cardiorespiratory fitness of an old, obese, female dwarf and a young, skinny, male giant of the same body weight. Although both have the same absolute VO2 max and the same relative VO2 max / weight, the relative VO2 max / height2 clearly shows that, despite the obesity of the female dwarf, she must have a much better cardiorespiratory fitness than the male giant to be able to reach the same oxygen consumption. Even if the dwarf and the giant would be of the same sex and age, the dwarf would still need to be in a much better cardiorespiratory condition (more efficient lungs, heart, blood/vessels, and muscle mitochondria) to be able to consume oxygen at the same rate as the giant. Therefore, the relative VO2 max / height2 (in L/min.m2) clearly is the only proper presentation of the VO2 max for comparing cardiorespiratory fitness independently of body size.
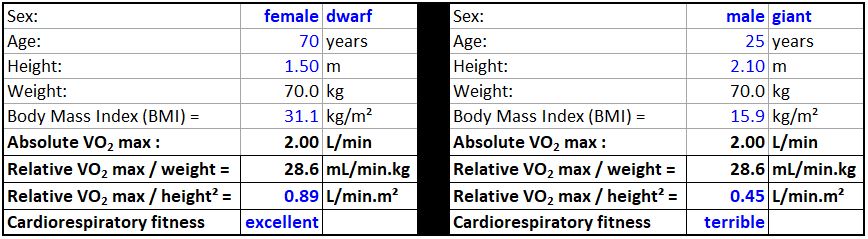
And indeed, with a BMI of 31 kg/m2, the dwarf is significantly overweight due to maybe extra muscle mass or more likely excess body fat. So, s/he could probably significantly improve general health and performance for distance running and cycling by losing some body fat. But that is a completely different issue and would not change her/his cardiorespiratory capacity. Similarly, with a BMI of only 16 kg/m2, the giant is significantly underweight and could probably significantly improve general health and strength by gaining some muscle mass and maybe some body fat. But again, that would not neccessarily change his/her cardiorespiratory capacity.
Side note: the broadly used body mass index (BMI=weight/height2 in kg/m2) suffers a similar disease as VO2 max because it is also incorrectly scaled for body size, giving taller individuals with exactly the same body shape and relative composition a larger BMI than shorter individuals. In alignment with the theory of geometric similarity, the corpulence index (CI= weight/height3 in kg/m3) is the correct way to normalize body weight for comparing people of different height.
For general health and fitness assessment, body mass (body weight), body composition (body fat versus lean mass), and cardiorespiratory fitness (maximum oxygen consumption) should be assessed separately / independently and compared to representative reference values that are properly scaled for body size to be able to understand where risks and opportunities are. This means body mass should be expressed by CI (in kg/m3), body composition should be expressed as relative body fat versus lean mass as a percentage of total body mass (in body fat% & lean mass%), and maximum oxygen consumption should be expressed as relative VO2 max / height2 (in L/min.m2) and compared to reference values from people of the same sex and age.
Information on my personal VO2 max result you can find in my photo blog.